
Due to the stress placed on the joint by short sprints, sudden stops, twists and turns, the knee is a common point of injury for tennis players. The cartilage known as the meniscus acts as a shock absorber between the thigh and shin bones and is therefore a ‘hotspot’ for damage in tennis players. Each knee has one lateral and one medial meniscus, either of which can be torn, and a tear can be quite painful, restricting movement considerably.
Even supreme athletes such as Roger Federer, can suffer from meniscus trouble. The Swiss star, who has won 20 Grand Slam titles, was forced to take time out of the game in 2016 when an MRI examination confirmed his fears of meniscal damage. You can read more about Federer’s injury and recovery here.
MRI is a good method for assessing deep intraarticular structures like the meniscus and articular cartilage. To evaluate articular cartilage injury, the radiologist must classify the stage and location of damage and in diagnosis of meniscal tears the radiologist must describe the location and spread of the rupture line.
Articular cartilage lesions look like a ‘gap’ in cartilage (arrow):

Meniscal tears look like linear disruption of the meniscus (arrow):
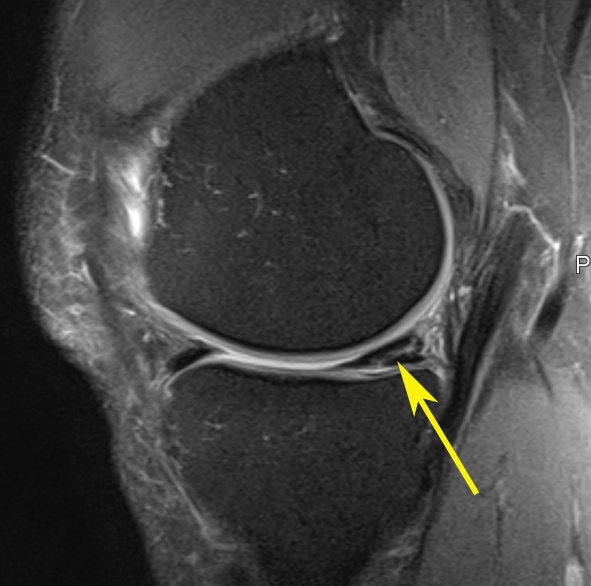
Note: images are examples – not those of the athlete named above.
MRI may not be the first imaging technique used to examine an injured knee, but in the case of soft tissue damage, it is often used to provide the most accurate visual assessment. The skill of the radiologist lies in being able to interpret the images and determine the exact nature of the tear. This information is crucial to the plan for treatment and recovery.
For more information about meniscus tears, click here.